Food is Medicine Fault Lines
“At one pole is a clinical, reimbursement-oriented, standardized worldview. At the other pole is a community-centered, systems-oriented, flexible worldview.” - C.J. Sentell, CEO
Every field reaches a point where its arguments stop being about tactics and start being about identity. Food Is Medicine (FIM) has largely arrived there. Beneath the visible debates — over terminology, evidence, eligibility, and sourcing — sits a single, deeper question: what kind of thing is Food Is Medicine, and whom does it serve?
After attending FIMCON in D.C. earlier this year, I wanted to understand how the key debates and conceptual tensions of the movement map onto its widely varying implementations. What I found is that these issues are not independent disputes but surface expressions of two coherent worldviews, and that understanding this structure clarifies where alliances are durable, where they are fragile, and where the field’s most generative opportunities lie.
Two poles
At one pole is a clinical, reimbursement-oriented, standardized worldview. It understands FIM as a medical intervention: food prescribed at the point of care to treat or manage diagnosed disease, validated by rigorous evidence, delivered to uniform standards, and ultimately paid for by health insurers. Its promise is durability and scale — a permanent place in the healthcare system.
At the other pole is a community-centered, systems-oriented, flexible worldview. It understands FIM as one component of a just food system: nourishing food connected to people through dignity and relationship, prioritizing local and equitable sourcing, prevention, and community engagement. Its promise is reach, legitimacy, and the capacity to address the conditions that produce diet-related disease in the first place.
Neither pole is wrong, and most organizations hold a blend of both. But nearly every contested choice in the field pulls toward one or the other, which is why the disagreements rhyme.
A quick way to locate a program’s orientation is to ask three questions: whom does it serve, how does it source, and what does it count as success? A program organized around becoming reimbursable will tend to serve the diagnosed, source by nutrient specification, and measure clinical and cost outcomes. A program organized around a particular community’s health will tend to serve by need, often source locally or regionally, and measure food security, trust, and reach. The three answers move together because they are driven by a single prior question — what the program is ultimately for. That motivation is the generative variable beneath the ten fault lines that follow; the columns are its visible signatures.
Importantly, motivation and position are not the same thing, which is what makes the fault lines worth thinking about. A program can be motivated by community health yet be pulled by funding structures toward the reimbursement pole — e.g., medically-tailored meal providers and produce-prescription programs that begin in the community and move into the payer world. It is worth paying attention to where a program’s heart sits and if, and how, its funding shapes its implementation.
The fault lines
Ten recurring fault lines run through the movement. Read down either column and a consistent posture emerges; the rows are not separate arguments so much as ten windows onto the same divide.
A structural note: these fault lines tend to travel together. Clinical integration correlates with sourcing-agnosticism (standardize the food to nutrition specifications and the lowest compliant supplier wins), while community-centered work correlates with local and equitable sourcing (the farm relationships are part of the point). The columns above are therefore best read as a single diagonal, not ten dials to be set independently.
How the field lines up
Plotting the major players against two axes — community-centered versus clinically integrated, and sourcing-agnostic versus equitable-sourcing-prioritized — makes the coalitions and rifts legible.
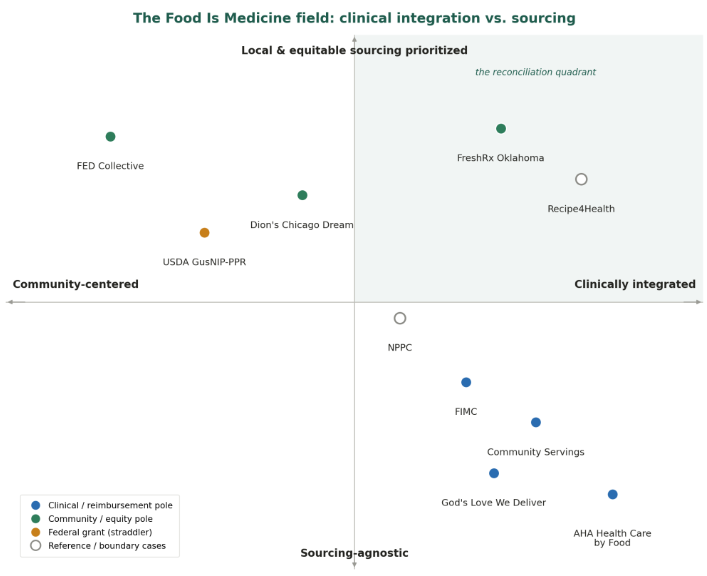
Major FIM organizations plotted by clinical integration (horizontal) and sourcing values (vertical). Color marks each organization's home pole; position marks where it actually operates — so the green markers in the upper-right reconciliation quadrant are community-rooted programs that have reached clinical integration. Hollow markers (Recipe4Health, NPPC) are reference points.
The American Heart Association’s Health Care by Food initiative is the purest expression of the clinical pole: a large, research-driven effort built to generate the randomized evidence that will make FIM a reimbursable medical benefit, essentially agnostic on where the food comes from. The Food is Medicine Coalition (FIMC) sits close beside it on standardization and reimbursement — it owns the field’s tightest accreditation criteria for medically tailored meals — but arrives there from the opposite origin: its members are CBO providers climbing into the clinical-payer world from community roots.
That shared destination is also the field’s most consequential latent rift. AHA and FIMC agree that FIM should be standardized, medically necessary, and reimbursed — but the moment reimbursement arrives, their interests can diverge over who sets quality standards, who is credentialed to deliver, and whether CBOs survive a payer market that rewards scale and low cost. The very mechanism that promises sustainability may narrow the mission that justified it.
The FED Collective — a group of BIPOC-led CBOs organized around the principles of fidelity, equity, and dignity — anchors the opposing pole. Crucially, it is not outside the movement in opposition; its framework was built specifically for the produce-prescription field. It is best understood as the equity conscience working from within, in tension with the clinical pole over gatekeeping, power, and sourcing rather than over whether FIM should exist. USDA’s produce-prescription work (the GusNIP program) is the quiet hinge between the poles: it funds the community and prevention end through grants while generating the standardized evaluation data that the reimbursement end depends on — building, somewhat ironically, the runway for the clinical world that may one day absorb it.
The diagonal predicts that one quadrant should be nearly vacant: organizations that are both clinically integrated and committed to local, equitable sourcing. That quadrant is where the field’s two worldviews would reconcile rather than split — and it is not entirely empty. Models such as Recipe4Health, a clinically integrated program embedded in federally qualified health centers and moving toward covered-benefit status, nonetheless write regenerative, local, and BIPOC-farmer sourcing into both their design and the coverage language they advocate. Such models are existence proofs that the diagonal is a tendency, not a law. For any organization rooted in the community-and-equity pole, this quadrant — not the clinical pole itself — is the strategically interesting frontier: it shows that a CBO can engage the reimbursement world without being flattened by it.
The pattern holds when more organizations are added. The medically-tailored-meal providers — e.g., God's Love We Deliver and Community Servings — sit beside FIMC in the clinical, standardized, sourcing-agnostic corner, as its member organizations would. Two cases complicate the diagonal in instructive ways. FreshRx Oklahoma, a produce prescription that pairs clinic referral and outcome tracking with local, regenerative, equity-driven sourcing, lands in the reconciliation quadrant — reaching it from the community side, just as Recipe4Health reached it from the clinical side. And Dion's Chicago Dream, a dignity-first, food-security-centered delivery model, has built a Medicaid-funded produce prescription channel that pulls it from the community pole toward the center — a community organization bridging into reimbursement.
Agency and Dignity
One further fault line deserves separate treatment, precisely because it does not travel on this diagonal: participant agency, or the degree of choice a program affords. At one end, food is prescribed with no selection — a medically tailored meal or a pre-packed produce box; at the other, participants choose freely, through farmers-market tokens or a produce-prescription card redeemed at retail, with curated boxes and delivery on one side and vouchers and cards on the other. What makes it distinct is that all four combinations exist: medically tailored meals are clinical and low-choice; a produce-prescription debit card is clinical but high-choice; farmers-market token programs are community-rooted and high-choice; and a curated box of local-farm produce is community-rooted yet low-choice. Because agency does not reduce to the clinical-versus-community divide, it is a semi-independent axis rather than another reading of the same one.
Its deeper significance is that it splits the idea of dignity itself — and the split runs inside the community-and-equity pole, not only between the poles. One reading of dignity is autonomy: people are not patients to be dosed, so let them choose, which favors vouchers and culturally relevant selection. The competing reading is dignity as access and quality: curate the best local, regenerative food, strip away the transportation and time barriers, and deliver it, which favors the box. These two dignities genuinely conflict, because tight local and regenerative sourcing from a handful of small farms often only works as a curated seasonal share — so maximizing choice tends to route programs through retail and cede the farm relationship, while maximizing equitable sourcing tends to constrain choice. A quieter force reinforces the same divide: a fixed box is a cleaner “dose” to study, so the clinical evidence agenda subtly favors controlled contents, while choice introduces the variability that complicates a trial.
Food insecurity & the clinical gateway
A question that looks merely administrative — must a participant be food insecure to receive FIM? — carries the entire clinical-versus-community divide inside it. Two terms do quiet work here. Food security measures quantity and access — whether a household reliably has enough food for an active, healthy life — and carries the anti-hunger, anti-poverty lineage of the safety net. Nutrition security is a newer framing centered on quality: consistent, affordable access to foods that actively promote health and prevent or treat disease. The shift is not merely additive — recasting the goal as nutrition security makes it legible to healthcare and to reimbursement, but it can also abstract hunger into a clinical risk factor and quietly displace the structural poverty that food insecurity names.
In practice, eligibility follows one of four logics. Most produce-prescription and medically-tailored grocery programs use a dual gate: a qualifying diet-related condition together with a positive food-insecurity screen. Many substitute a proxy, treating enrollment in a means-tested program such as Medicaid or SNAP as evidence of food insecurity. Some require a clinical diagnosis alone, with no food-access test — the medically-tailored-meal tradition and the framing favored by the clinical pole, where the warrant is the disease rather than household budget. And some, mostly in the grant-funded CBO world, require food insecurity alone (or residence in a high-need area) with no clinical gate at all.
Beneath the variation sits a collision between two logics of who deserves the benefit. Food insecurity is a social and economic criterion; medical necessity — the gateway to insurance reimbursement — is a clinical one, and by law a permanent Medicaid benefit generally cannot single out particular conditions or means-test medical care the way an anti-poverty program does. The community pole targets the food insecure precisely because they are the people for whom food access, not diagnosis, is the binding constraint. So the eligibility question is actually a proxy for another, deeper question: is FIM medical treatment or social policy?
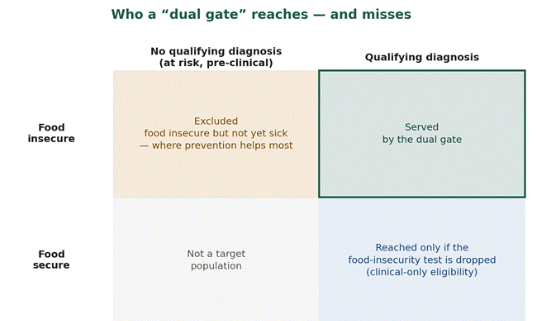
A dual gate serves only those who clear both tests, and misses the food insecure who are not yet sick. A proxy such as Medicaid or SNAP enrollment shifts the dividing line toward insurance status.
The concept doing the work here is “health-related social needs” (HRSN). This is the term the healthcare system uses to reclassify non-medical conditions — food, housing, transportation, interpersonal safety — as health-relevant, and therefore as something payers can be asked to cover. Health-related social needs are the conceptual bridge across the central divide: they are the mechanism by which a community concern like hunger becomes a reimbursable medical service. That makes it the field’s most consequential policy instrument — the door to the reconciliation quadrant, where Medicaid pays CBOs to do FIM work — but it opens that door on the clinical pole’s terms, medicalized and dual-gated. Its partial retraction in 2025, then, is not a technicality; it is the field’s central tension playing out in real time, deciding whether the social and the clinical can be funded as one thing or must split apart again.
The dominant federal pathway tried to split the difference, and in doing so revealed which way the field is tilting. Under the Centers for Medicare and Medicaid Services’ Health-Related Social Needs framework for Section 1115 waivers, nutrition supports were offered only to enrollees who were medically appropriate and met both clinical and social risk-factor criteria — a dual gate, but one in which hunger was reframed as “nutrition insecurity,” and the services were positioned as treatments for defined patient populations rather than as programs addressing poverty. Even where food insecurity survives as a criterion, the framing battle is being won by the clinical worldview. Nor is the ground stable: in March 2025 the federal guidance underwriting that framework was rescinded, leaving existing approvals intact but future social-need coverage to be decided case by case — throwing weight back onto grant funding and state improvisation, and reopening the eligibility question rather than settling it.
The consequences are significant, and in places perverse. The dual gate — diagnosis and food-insecurity screen together — is the most exclusionary design of all, and it cuts directly against prevention: it cannot reach the food insecure who are not yet sick, the very people upstream help would serve best for public health goals. Proxies ease the screening burden but redraw the boundary of “the deserving” around insurance status, excluding the food insecure who are uninsured, just above the income line, or barred from Medicaid by immigration status, while including enrollees who are not currently in need. And if reimbursement pressure pushes the field toward clinical-only eligibility, the benefit can drift up the income gradient toward insured, diagnosed, comparatively better-off patients — an equity failure hidden inside a scalability win. For an organization that treats food security as the very point of its work, this is the eligibility-level form of the field’s central choice: keep food insecurity central and remain in the equity lane, harder to reimburse, or adopt clinical eligibility to reach reimbursement and risk drifting from the people it exists to serve.
Why the fault lines matter
Read as a single structure, rather than a list of policy choices, these tensions become predictive, explaining in advance which alliances will hold, which will fracture, and why. They explain why allies who agree on the goal can still collide over implementation, why the grant world and the reimbursement world are more entangled than they appear, and why the contest over sourcing is ultimately an argument about whether FIM is a narrow health intervention or a broader instrument of food-system change through the lens of public health.
The most important strategic questions for the field follow directly: Can the clinical pole’s drive for evidence and reimbursement be harnessed without surrendering community ownership and equitable sourcing? Can standardization and local autonomy be reconciled in a single accreditation logic? Must a person be hungry to deserve nourishing food as care — or sick to deserve it at all? And who will occupy the reconciliation quadrant in numbers, proving that the movement’s two worlds can in fact be one?
These questions matter because the fault lines in the FIM movement reveal deeper institutional pressures. Reimbursement rules shape eligibility. Evidence standards shape intervention design. Agricultural policy shapes what food is grown, what it costs, and whose farms survive. Community organizations, health systems, funders, and policymakers are not simply choosing among neutral alternatives; they are responding to incentives built into larger economic and political systems. Recognizing this does not make the movement's internal debates less important. It makes them more consequential. Every decision about evidence, sourcing, eligibility, or delivery quietly answers a larger question about what FIM is becoming—and whether it will merely treat the consequences of a broken food system or help reshape the conditions that made it necessary in the first place.
Beyond FIM
The framework presented here also points beyond FIM itself. The movement did not create the conditions it now seeks to address. Rising rates of diet-related disease reflect decades of choices about agricultural subsidies, food manufacturing, labor markets, housing, health care, transportation, education, and economic opportunity. Likewise, the movement's internal fault lines are not simply products of competing philosophies; they are shaped by reimbursement systems, philanthropic priorities, regulatory structures, and political incentives that reward some approaches while constraining others.
Seen this way, FIM is less a complete solution than a revealing intervention. It exposes the places where healthcare, agriculture, and social policy fail to align. No single reimbursement model, produce prescription, or medically tailored meal program can resolve those underlying contradictions. Human flourishing ultimately depends on a broader ecosystem of institutions: a food system that rewards nutritious production rather than simply inexpensive calories; healthcare that values prevention alongside treatment; labor policies that provide living wages; housing and transportation that make healthy food accessible; and communities with the capacity to shape their own food futures.
The question, then, is not whether FIM should become more clinical or more community-centered. It is whether the movement can hold these commitments together while building a world in which food is once again ordinary nourishment rather than extraordinary medicine.